
Hemodialysis
While healthy kidneys have several functions in the body, the most well-known job is to produce urine. When kidney function goes below 10% to 15% kidneys are no longer able to filter the blood and make urine. This causes toxins to build up in the body along with excess fluid. Fortunately, we live in a time when there are treatments and medicines that can replace the functions of the kidneys and keep the body alive. One type of renal replacement therapy — meaning a treatment that replaces kidney function — is hemodialysis. Hemodialysis is a therapy that filters waste, removes extra fluid and balances electrolytes (sodium, potassium, bicarbonate, chloride, calcium, magnesium and phosphate).
How is hemodialysis done?
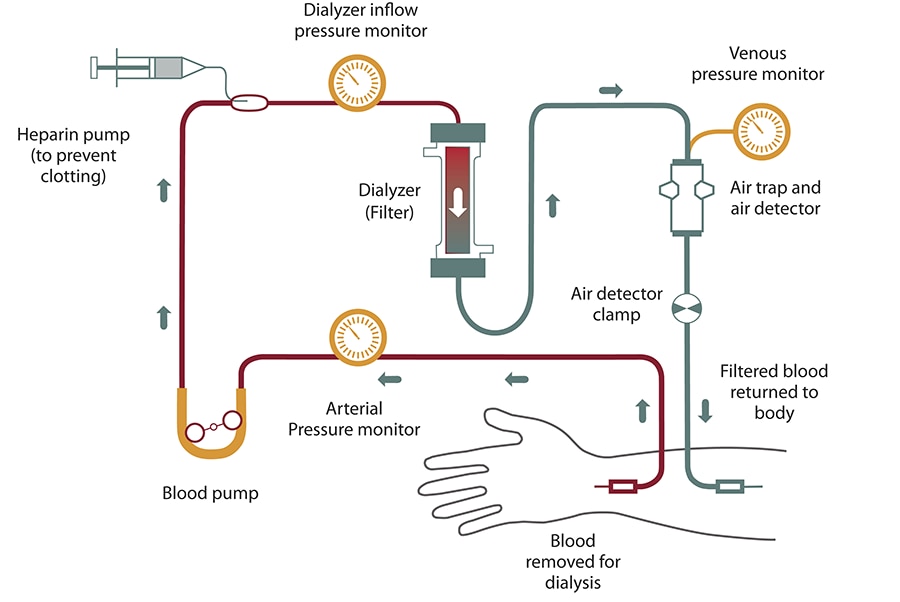
In hemodialysis, blood is removed from the body and filtered through a man-made membrane called a dialyzer, or artificial kidney, and then the filtered blood is returned to the body. The average person has about 10 to 12 pints of blood; during dialysis only one pint (about two cups) is outside of the body at a time. To perform hemodialysis there needs to be an access created to get the blood from the body to the dialyzer and back to the body. There are three access types for hemodialysis: arteriovenous (AV) fistula, AV graft and central venous catheter. The AV fistula is the vascular access most recommended by the dialysis community; however, you and your doctor will decide which access is best for you.
When a patient goes to hemodialysis, a nurse or technician will check vital signs and get the patient’s weight. The weight gain will tell how much excess fluid the patient has to have removed during the treatment. The patient is then “put on the machine”. Patient with a vascular access (AV fistula or AV graft) will get two needle sticks in their access; one needle takes blood out of the body, the other needle puts it back. Patients with a central venous catheter will have the two tubes from their access connected to the blood tubes that lead to the dialyzer and back to the body. Once the patient is “put on the machine”, the dialysis machine is programmed and then treatment begins.
Blood never actually goes through the dialysis machine. The dialysis machine is like a big computer and a pump. It keeps track of blood flow, blood pressure, how much fluid is removed and other vital information. It mixes the dialysate, or dialysis solution, which is the fluid bath that goes into the dialyzer. This fluid helps pull toxins from the blood, and then the bath goes down the drain. The dialysis machine has a blood pump that keeps the blood flowing by creating a pumping action on the blood tubes that carry the blood from the body to the dialyzer and back to the body. The dialysis machine also has many safety detection features. If you visit a dialysis center, you will likely hear some of the warning sounds made by a dialysis machine.
How does hemodialysis work?
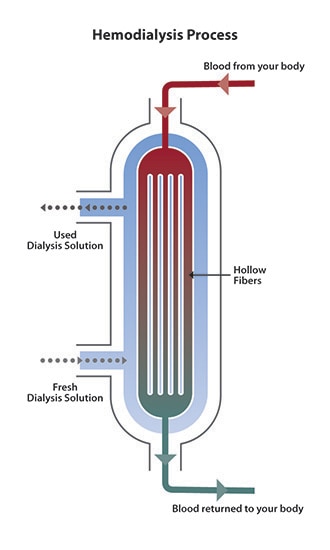
The dialyzer is the key to hemodialysis. The dialyzer is called the artificial kidney because it filters the blood — a job the kidneys used to do. The dialyzer is a hollow plastic tube about a foot long and three inches in diameter that contains many tiny filters. (Dialyzers are made in different sizes so doctors can prescribe the best one for their patients.) There are two sections in the dialyzer; the section for dialysate and the section for the blood. The two sections are divided by a semipermeable membrane so that they don’t mix together. A semipermeable membrane has microscopic holes that allow only some substances to cross the membrane. Because it is semipermeable, the membrane allows water and waste to pass through, but does not allow blood cells to pass through.
Dialysate, also called dialysis fluid, dialysis solution or bath, is a solution of pure water, electrolytes and salts, such as bicarbonate and sodium. The purpose of dialysate is to pull toxins from the blood into the dialysate. The way this works is through a process called diffusion. In the blood of the hemodialysis patient, there is a high concentration of waste, while the dialysate has a low concentration of waste. Due to the difference in concentration, the waste will move through the semipermeable membrane to create an equal amount on both sides. The dialysis solution is then flushed down the drain along with the waste. The electrolytes in the dialysis solution are also used to balance the electrolytes in the patient’s blood. The extra fluid is removed through a process called filtration. The fluid is pushed off by higher pressure on the blood side than on the dialysate side.
How often is hemodialysis done?
Blood needs to flow through the dialyzer for several hours to adequately clean the blood and rid the body of excess fluid. Traditional, in-center hemodialysis is generally done three times a week for about four hours each session. Your doctor will prescribe how long your treatments will be, usually between 3 to 5 hours, but most common is 4 hours. Talk to your doctor about how long you should be on hemodialysis. Some people feel that dialysis lasts a long time; however, healthy kidneys work 24 hours a day, 7 days a week and dialysis must do the job in only 12 or so hours a week.
Alternative hemodialysis schedules include nocturnal and short daily. Normally, these treatments are performed by people who do home hemodialysis. With nocturnal hemodialysis, the patient has dialysis for about eight hours overnight while sleeping. This is a longer, gentler treatment so patients say they have fewer problems with cramping and the “washed out” feeling reported after traditional hemodialysis. More dialysis centers are beginning to offer in-center nocturnal hemodialysis based on reports of patients feeling better about their quality of life and having good lab results. Short daily hemodialysis is performed five or six times per week for about two to three hours each treatment. Talk to your doctor if you are interested in home hemodialysis (HHD) or in-center nocturnal dialysis. You may want to ask your social worker if addition treatments, such as the longer nocturnal hemodialysis and short daily hemodialysis will be covered through your insurance.
Advantages and disadvantages of hemodialysis
Hemodialysis is an effective treatment for those with end stage renal disease. However, hemodialysis alone will not provide a complete treatment for those with kidney failure. Diet and fluid restrictions need to be followed, and medicines may need to be taken to replace other functions of the kidneys, such as regulating blood pressure and stimulating production of red blood cells to prevent anemia.
For those who choose in-center hemodialysis, some of the benefits are that they will have their treatments performed in a dialysis center by trained professionals. They can spend their time in dialysis sleeping, reading, writing, watching television, listening to music or doing other quiet activities. There are four days a week when they will not have to go to dialysis. Some of the disadvantages are that they will have to travel to and from hemodialysis three times each week and it takes advanced notice to travel and arrange for dialysis in a visiting dialysis center. The diet restrictions include limiting foods that contain phosphorus, potassium and sodium and drinking a limited amount of fluid. Some people report a “washed out” feeling after hemodialysis and go home to take a nap. Those who perform nocturnal hemodialysis (in center or at home) report that this washed out feeling is not as common. Also, because nocturnal dialysis is performed during nonproductive sleeping hours, many people report they feel that their lives are more “normal” because they don’t have to take time out of their days for dialysis.
People who choose to perform hemodialysis at home say they enjoy the feeling of control they have over their lives. Instead of going to the dialysis center at a certain time, they can choose when to perform hemodialysis around their schedule.
Risks
Most people who require hemodialysis have a variety of health problems. Hemodialysis prolongs life for many people, but life expectancy for people who need it is still less than that of the general population.
While hemodialysis treatment can be efficient at replacing some of the kidney's lost functions, you may experience some of the related conditions listed below, although not everyone experiences all of these issues. Your dialysis team can help you deal with them.
- Low blood pressure (hypotension). A drop in blood pressure is a common side effect of hemodialysis, particularly if you have diabetes. Low blood pressure may be accompanied by shortness of breath, abdominal cramps, muscle cramps, nausea or vomiting.
- Muscle cramps. Although the cause is not clear, muscle cramps during hemodialysis are common. Sometimes the cramps can be eased by adjusting the hemodialysis prescription. Adjusting fluid and sodium intake between hemodialysis treatments also may help prevent symptoms during treatments.
- Itching. Many people who undergo hemodialysis have itchy skin, which is often worse during or just after the procedure.
- Sleep problems. People receiving hemodialysis often have trouble sleeping, sometimes because of breaks in breathing during sleep (sleep apnea) or because of aching, uncomfortable or restless legs.
- Anemia. Not having enough red blood cells in your blood (anemia) is a common complication of kidney failure and hemodialysis. Failing kidneys reduce production of a hormone called erythropoietin (uh-rith-roe-POI-uh-tin), which stimulates formation of red blood cells. Diet restrictions, poor absorption of iron, frequent blood tests, or removal of iron and vitamins by hemodialysis also can contribute to anemia.
- Bone diseases. If your damaged kidneys are no longer able to process vitamin D, which helps you absorb calcium, your bones may weaken. In addition, overproduction of parathyroid hormone — a common complication of kidney failure — can release calcium from your bones.
- High blood pressure (hypertension). If you consume too much salt or drink too much fluid, your high blood pressure is likely to get worse and lead to heart problems or strokes.
- Fluid overload. Since fluid is removed from your body during hemodialysis, drinking more fluids than recommended between hemodialysis treatments may cause life-threatening complications, such as heart failure or fluid accumulation in your lungs (pulmonary edema).
- Inflammation of the membrane surrounding the heart (pericarditis). Insufficient hemodialysis can lead to inflammation of the membrane surrounding your heart, which can interfere with your heart's ability to pump blood to the rest of your body.
- High potassium levels (hyperkalemia). Potassium is a mineral that is normally removed from your body by your kidneys. If you consume more potassium than recommended, your potassium level may become too high. In severe cases, too much potassium can cause your heart to stop.
- Access site complications. Potentially dangerous complications ― such as infection, narrowing or ballooning of the blood vessel wall (aneurysm), or blockage ― can impact the quality of your hemodialysis. Follow your dialysis team's instructions on how to check for changes in your access site that may indicate a problem.
- Amyloidosis. Dialysis-related amyloidosis develops when proteins in blood are deposited on joints and tendons, causing pain, stiffness and fluid in the joints. The condition is more common in people who have undergone hemodialysis for more than five years.
- Depression. Changes in mood are common in people with kidney failure. If you experience depression or anxiety after starting hemodialysis, talk with your health care team about effective treatment options.
How you prepare
Preparation for hemodialysis starts several weeks to months before your first procedure. To allow for easy access to your bloodstream, a surgeon will create a vascular access. The access provides a mechanism for a small amount of blood to be safely removed from your circulation and then returned to you in order for the hemodialysis process to work. The surgical access needs time to heal before you begin hemodialysis treatments.
There are three types of accesses:
- Arteriovenous (AV) fistula. A surgically created AV fistula is a connection between an artery and a vein, usually in the arm you use less often. This is the preferred type of access because of effectiveness and safety.
- AV graft. If your blood vessels are too small to form an AV fistula, the surgeon may instead create a path between an artery and a vein using a flexible, synthetic tube called a graft.
- Central venous catheter. If you need emergency hemodialysis, a plastic tube (catheter) may be inserted into a large vein in your neck or near your groin. The catheter is temporary.
You can receive hemodialysis in a dialysis center, at home or in a hospital. The frequency of treatment varies, depending on your situation:
- In-center hemodialysis. Many people get hemodialysis three times a week in sessions of three to five hours each.
- Daily hemodialysis. This involves more-frequent, but shorter sessions — usually performed at home six or seven days a week for about two to three hours each time.
Simpler hemodialysis machines have made home hemodialysis less cumbersome, so with special training and someone to help you, you may be able to do hemodialysis at home. You may even be able to do the procedure at night while you sleep.
There are dialysis centers located throughout the United States and in some other countries, so you can travel to many areas and still receive your hemodialysis on schedule. Your dialysis team can help you make appointments at other locations, or you can contact the dialysis center at your destination directly. Plan ahead to make sure space is available and proper arrangements can be made.
The procedure
During treatments, you sit or recline in a chair while your blood flows through the dialyzer ― a filter that acts as an artificial kidney to clean your blood. You can use the time to watch TV or a movie, read, nap, or perhaps talk to your "neighbors" at the center. If you receive hemodialysis at night, you can sleep during the procedure.
- Preparation. Your weight, blood pressure, pulse and temperature are checked. The skin covering your access site — the point where blood leaves and then re-enters your body during treatment — is cleansed.
- Starting. During hemodialysis, two needles are inserted into your arm through the access site and taped in place to remain secure. Each needle is attached to a flexible plastic tube that connects to a dialyzer. Through one tube, the dialyzer filters your blood a few ounces at a time, allowing wastes and extra fluids to pass from your blood into a cleansing fluid called dialysate. The filtered blood returns to your body through the second tube.
- Symptoms. You may experience nausea and abdominal cramps as excess fluid is pulled from your body — especially if you have hemodialysis only three times a week rather than more often. If you're uncomfortable during the procedure, ask your care team about minimizing side effects by such measures as adjusting the speed of your hemodialysis, your medication or your hemodialysis fluids.
- Monitoring. Because blood pressure and heart rate can fluctuate as excess fluid is drawn from your body, your blood pressure and heart rate will be checked several times during each treatment.
- Finishing. When hemodialysis is completed, the needles are removed from your access site and a pressure dressing is applied to prevent bleeding. Your weight may be recorded again. Then you're free to go about your usual activities until your next session.
Results
If you had sudden (acute) kidney injury, you may need hemodialysis only for a short time until your kidneys recover. If you had reduced kidney function before a sudden injury to your kidneys, the chances of full recovery back to independence from hemodialysis are lessened.
Although in-center, three-times-a-week hemodialysis is more common, some research suggests that home dialysis is linked to:
- Better quality of life
- Increased well-being
- Reduced symptoms and less cramping, headaches and shortness of breath
- Improved appetite, sleeping patterns, energy level and ability to concentrate
Your hemodialysis care team monitors your treatment to make sure you're getting the right amount of hemodialysis to remove enough wastes from your blood. Your weight and blood pressure are monitored very closely before, during and after your treatment. About once a month, you'll receive these tests:
- Blood tests to measure urea reduction ratio (URR) and total urea clearance (Kt/V) to see how well your hemodialysis is removing waste from your body
- Blood chemistry evaluation and assessment of blood counts
- Measurements of the flow of blood through your access during hemodialysis
Your care team may adjust your hemodialysis intensity and frequency based, in part, on test results.
Between treatments
Between hemodialysis treatments you can help achieve the best possible results from your hemodialysis by:
- Eating the right foods. Eating properly can improve your hemodialysis results and your overall health. While you're receiving hemodialysis, you'll need to carefully monitor your intake of fluids, protein, sodium, potassium and phosphorus. A dietitian can help you develop an individualized meal plan based on your weight, personal preferences, remaining kidney function and other medical conditions, such as diabetes or high blood pressure.
- Taking your medications as prescribed. Carefully follow the instructions from your health care team.
- Allowing your team to assist you by discussing your concerns. Your health care team can present options to you and help you deal with any concerns.
- Biochemical mechanisms involved in blood-hemodialysis membrane interactions
- Clinical consequences of hemodialysis membrane biocompatibility
- Complications of hemodialysis in the older patient
- Contaminants in water used for hemodialysis
- Hemodialysis in the older adult
- Maintaining water quality for hemodialysis
- Overview of the hemodialysis apparatus
- Plasmapheresis with hemodialysis equipment
- Psychiatric illness in dialysis patients
- Reactions to the hemodialysis membrane
- Reuse of dialyzers
- Serum enzymes in patients with renal failure
- Ultrapure dialysis fluid
- Water purification systems in hemodialysis
Related Conference of Hemodialysis
14th European Congress on Nephrology, Internal Medicine and Kidney Diseases
Hemodialysis Conference Speakers
Recommended Sessions
- Acute Renal Failure and Dialysis
- Anemia and Chronic Renal Failure
- Cardiac Disease and Hypertension
- Complications during Dialysis
- Dialysis Adequacy
- Dialysis Modalities
- Endocrine Dysfunction
- Hemodialysis
- Infection and Dialysis
- Intoxications
- Nutrition
- Other
- Peritoneal Dialysis
- Slow Continuous Therapies
- Vascular access
Related Journals
Are you interested in
- Acute Kidney Injury (AKI) - Kidney Care 2027 (UK)
- Acute Kidney Injury (AKI) & Critical Care Nephrology - EURO NEPHROLOGY 2026 (Germany)
- Acute Kidney Injury and Critical Care Nephrology - World Nephrology 2027 (Netherlands)
- Acute Kidney Injury Mechanisms and Management - UROLOGY 2026 (Spain)
- Aging Populations and Geriatric Epidemiology - EPIDEMIOLOGY-2026 (Netherlands)
- Aging, Frailty, and Geriatric Nephrology - World Nephrology 2027 (Netherlands)
- Artificial Intelligence & Digital Nephrology - EURO NEPHROLOGY 2026 (Germany)
- Artificial Intelligence and Digital Nephrology - World Nephrology 2027 (Netherlands)
- Artificial Intelligence in Nephrology - Kidney Care 2027 (UK)
- Benign Urological Conditions and Management - UROLOGY 2026 (Spain)
- Biomarkers and Translational Kidney Research - World Nephrology 2027 (Netherlands)
- Biomarkers in Kidney Disease - Kidney Meet 2026 (Japan)
- Biomarkers of Kidney Diseases - Euro Nephrology Summit 2026 (France)
- Biomarkers, Imaging & Diagnostics in Nephrology - EURO NEPHROLOGY 2026 (Germany)
- Cardio-Renal Syndrome - World Nephrology 2027 (Netherlands)
- Cardiorenal Syndrome - Euro Nephrology Summit 2026 (France)
- Cardiovascular and Kidney Health - Kidney Care 2027 (UK)
- Cardiovascular Impact of Kidney Disease - Kidney Meet 2026 (Japan)
- Chronic Kidney Disease - Kidney Meet 2026 (Japan)
- Chronic Kidney Disease (CKD) - Kidney Care 2027 (UK)
- Chronic Kidney Disease (CKD) – Early Detection & Prevention - EURO NEPHROLOGY 2026 (Germany)
- Chronic Kidney Disease (CKD): Prevention and Management - World Nephrology 2027 (Netherlands)
- Climate Change and Environmental Health - EPIDEMIOLOGY-2026 (Netherlands)
- Clinical Nephrology - Euro Nephrology Summit 2026 (France)
- Clinical Trials and Emerging Therapies in Nephrology - World Nephrology 2027 (Netherlands)
- Clinical Trials and Translational Nephrology - Kidney Care 2027 (UK)
- Clinical Trials and Translational Research - UROLOGY 2026 (Spain)
- Critical Care Nephrology - Kidney Meet 2026 (Japan)
- Diabetic and Hypertensive Kidney Disease - UROLOGY 2026 (Spain)
- Diabetic Kidney Disease - World Nephrology 2027 (Netherlands)
- Diabetic Kidney Disease - Kidney Care 2027 (UK)
- Diabetic Kidney Disease & Metabolic Disorders - EURO NEPHROLOGY 2026 (Germany)
- Diabetic Nephropathy - Euro Nephrology Summit 2026 (France)
- Diabetic Nephropathy - Kidney Meet 2026 (Japan)
- Diagnostic, Imaging and Radiation Techniques - Euro Nephrology Summit 2026 (France)
- Dialysis - Kidney Meet 2026 (Japan)
- Dialysis and Renal Replacement Therapies - Kidney Care 2027 (UK)
- Dialysis Innovations and Renal Replacement Therapy - World Nephrology 2027 (Netherlands)
- Dialysis Technologies & Renal Replacement Therapy - EURO NEPHROLOGY 2026 (Germany)
- Diet for Kidney Health - Euro Nephrology Summit 2026 (France)
- Digital Health and Artificial Intelligence Applications - UROLOGY 2026 (Spain)
- Digital Health and Epidemiological Data Science - EPIDEMIOLOGY-2026 (Netherlands)
- Digital Health and Tele-Nephrology - Kidney Care 2027 (UK)
- Drugs used in the treatment of Kidney Diseases - Euro Nephrology Summit 2026 (France)
- Environmental and Occupational Kidney Diseases - World Nephrology 2027 (Netherlands)
- Epidemiology and Global Burden of Renal and Urological Disorders - UROLOGY 2026 (Spain)
- Foundations of Urology and Nephrology - UROLOGY 2026 (Spain)
- Future Directions in Urology and Nephrological Disorders - UROLOGY 2026 (Spain)
- Future Perspectives in Nephrology and Renal Innovation - World Nephrology 2027 (Netherlands)
- Genetic and Inherited Kidney Diseases - Kidney Care 2027 (UK)
- Genetic and Rare Kidney Diseases - World Nephrology 2027 (Netherlands)
- Genetics and Molecular Basis of Kidney and Urological Diseases - UROLOGY 2026 (Spain)
- Genomic Epidemiology and Precision Public Health - EPIDEMIOLOGY-2026 (Netherlands)
- Geriatric Nephrology - Kidney Care 2027 (UK)
- Geriatric Nephrology & Aging Kidneys - EURO NEPHROLOGY 2026 (Germany)
- Geriatric Urology and Renal Health - UROLOGY 2026 (Spain)
- Global Epidemiology and Disease Surveillance - EPIDEMIOLOGY-2026 (Netherlands)
- Global Kidney Health and Public Health - Kidney Care 2027 (UK)
- Global Kidney Health and Public Health Policies - World Nephrology 2027 (Netherlands)
- Glomerular Disease - Euro Nephrology Summit 2026 (France)
- Glomerular Diseases - Kidney Care 2027 (UK)
- Glomerular Diseases & Autoimmune Nephrology - EURO NEPHROLOGY 2026 (Germany)
- Glomerular Diseases and Autoimmune Nephrology - World Nephrology 2027 (Netherlands)
- Health Systems and Policy Research - EPIDEMIOLOGY-2026 (Netherlands)
- Hematology in Kidney Health - Kidney Meet 2026 (Japan)
- Hereditary Kidney Disorders - Euro Nephrology Summit 2026 (France)
- Hypertension & Cardio-Renal Syndrome - EURO NEPHROLOGY 2026 (Germany)
- Hypertension and Kidney Health - Kidney Meet 2026 (Japan)
- Hypertension and Renal Disorders - World Nephrology 2027 (Netherlands)
- Hypertension and Renal Disorders - Kidney Care 2027 (UK)
- Hypertension associated with Kidney Diseases - Euro Nephrology Summit 2026 (France)
- Imaging and Diagnostics in Urology and Nephrology - UROLOGY 2026 (Spain)
- Infectious Diseases and Pandemic Preparedness - EPIDEMIOLOGY-2026 (Netherlands)
- Innovations and Future Directions in Kidney Care - Kidney Care 2027 (UK)
- Interventional Nephrology - World Nephrology 2027 (Netherlands)
- Interventional Nephrology - Kidney Care 2027 (UK)
- Kidney Cancer and Onco-Nephrology - World Nephrology 2027 (Netherlands)
- Kidney Cancer and Onco-Nephrology - Kidney Care 2027 (UK)
- Kidney Failure - Kidney Meet 2026 (Japan)
- Kidney Stones - Euro Nephrology Summit 2026 (France)
- Kidney Stones - Kidney Meet 2026 (Japan)
- Kidney Transplantation - Euro Nephrology Summit 2026 (France)
- Kidney Transplantation - Kidney Meet 2026 (Japan)
- Kidney Transplantation - Kidney Care 2027 (UK)
- Kidney Transplantation & Transplant Immunology - EURO NEPHROLOGY 2026 (Germany)
- Kidney Transplantation and Immunology - World Nephrology 2027 (Netherlands)
- Kidney Transplantation Science and Practice - UROLOGY 2026 (Spain)
- Lifestyle Factors and Preventive Urology and Nephrology - UROLOGY 2026 (Spain)
- Maternal and Child Health Epidemiology - EPIDEMIOLOGY-2026 (Netherlands)
- Maternal and Child Health Epidemiology - EPIDEMIOLOGY-2026 (Netherlands)
- Mental Health and Behavioral Epidemiology - EPIDEMIOLOGY-2026 (Netherlands)
- Migration, Displacement, and Global Health - EPIDEMIOLOGY-2026 (Netherlands)
- Mineral and Bone Disorders in CKD - Kidney Meet 2026 (Japan)
- Minimally Invasive and Robotic Urological Surgery - UROLOGY 2026 (Spain)
- Nephrology - Euro Nephrology Summit 2026 (France)
- Nephrology Nursing - Kidney Meet 2026 (Japan)
- Nephrology Nursing - Kidney Care 2027 (UK)
- Nephrology Nursing and Patient Care - World Nephrology 2027 (Netherlands)
- Nephrotic Syndrome - Euro Nephrology Summit 2026 (France)
- Non-Communicable Diseases: Prevention and Control - EPIDEMIOLOGY-2026 (Netherlands)
- Nutrition and Lifestyle in Kidney Health - World Nephrology 2027 (Netherlands)
- Nutrition and Public Health - EPIDEMIOLOGY-2026 (Netherlands)
- Occupational and Industrial Epidemiology - EPIDEMIOLOGY-2026 (Netherlands)
- Pathophysiology of Chronic Kidney Disease - UROLOGY 2026 (Spain)
- Patient-Centered Care, Quality of Life & Ethics - EURO NEPHROLOGY 2026 (Germany)
- Pediatric and Geriatric Nephrology - Kidney Meet 2026 (Japan)
- Pediatric Nephrology - Euro Nephrology Summit 2026 (France)
- Pediatric Nephrology - World Nephrology 2027 (Netherlands)
- Pediatric Nephrology - Kidney Care 2027 (UK)
- Pediatric Nephrology & Congenital Kidney Diseases - EURO NEPHROLOGY 2026 (Germany)
- Pediatric Urology and Nephrology - UROLOGY 2026 (Spain)
- Pharmacological Approaches in Kidney Disease - Kidney Meet 2026 (Japan)
- Precision and Personalized Medicine in Renal and Urological Care - UROLOGY 2026 (Spain)
- Precision Medicine & Genetic Kidney Disorders - EURO NEPHROLOGY 2026 (Germany)
- Precision Medicine in Nephrology - World Nephrology 2027 (Netherlands)
- Precision Nephrology - Kidney Care 2027 (UK)
- Public Health Preparedness and Emergency Response - EPIDEMIOLOGY-2026 (Netherlands)
- Public Health, Epidemiology & Global Kidney Care - EURO NEPHROLOGY 2026 (Germany)
- Regenerative Medicine and Stem Cell Therapy - World Nephrology 2027 (Netherlands)
- Regenerative Medicine and Stem Cell Therapy - Kidney Care 2027 (UK)
- Renal Imaging and Diagnostics - Kidney Care 2027 (UK)
- Renal Nutrition - Kidney Meet 2026 (Japan)
- Renal Nutrition and Dietetics - Kidney Care 2027 (UK)
- Renal Nutrition, Lifestyle & Preventive Care - EURO NEPHROLOGY 2026 (Germany)
- Renal Pathology - Kidney Care 2027 (UK)
- Renal Pathology and Diagnostic Innovations - World Nephrology 2027 (Netherlands)
- Renal Pathology and Immunology - Kidney Meet 2026 (Japan)
- Renal Pharmacology and Therapeutics - World Nephrology 2027 (Netherlands)
- Renal Pharmacology and Therapeutics - Kidney Care 2027 (UK)
- Renal Replacement Therapy and Dialysis Innovations - UROLOGY 2026 (Spain)
- Robotic Kidney Transplantation - Kidney Meet 2026 (Japan)
- Social Determinants of Health and Health Equity - EPIDEMIOLOGY-2026 (Netherlands)
- Stages of Kidney Diseases - Euro Nephrology Summit 2026 (France)
- Stem cells in Renal Disorders - Euro Nephrology Summit 2026 (France)
- Stem Cells in Renal Disorders - Kidney Meet 2026 (Japan)
- Technological Advancements in Nephrology - Euro Nephrology Summit 2026 (France)
- Urinary Tract Infections and Inflammatory Disorders - UROLOGY 2026 (Spain)
- Urological Oncology Advances - UROLOGY 2026 (Spain)
- Urology - Kidney Meet 2026 (Japan)
- Women's Kidney Health - Kidney Care 2027 (UK)
- Women’s Health and Pregnancy - Kidney Meet 2026 (Japan)
- Women’s Kidney Health - World Nephrology 2027 (Netherlands)